
Speech Therapy for Down Syndrome is quite Unique
Children with Down Syndrome are truly unique in the way that they communicate and interact. Treating these children can often be difficult because this syndrome involves so many different developmental domains, such as:
- Anatomical and physical differences, such as low tone and a high narrow palate relative to tongue size.
- Typically, there can be a high desire for social-emotional interaction.
- Motor planning limitations such as weak posture and low strength can occur but at the same time a child can have a highly functional vocabulary of gestures.
- Strong receptive language skills are often common alongside limited expressive language.
- There can also be reduced or fluctuating hearing.
It makes sense that 1) because this population is different and 2) because Down Syndrome is common enough, that there would be strategies for speech therapy for Down Syndrome that take these unique characteristics into consideration.
This is where Total Communication comes in. Total Communication basically means:
Give speech therapy through verbal AND other modalities such as visual, auditory, kinesthetic, and tactile awareness.
This could include signing, visual manipulatives, as well as voice output devices. The point is that many communication strategies, when used together, produce much greater results.
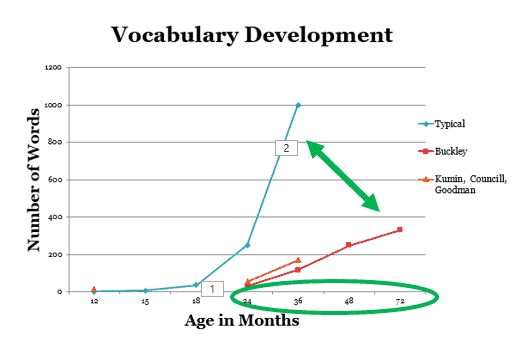
And here’s why: In studies of vocabulary, children with Down Syndrome not only experience a later start to vocabulary acquisition but slower growth over time.
With regards to language development, early milestones are nearly equal, while peers with typical development develop rapidly after 12 months.
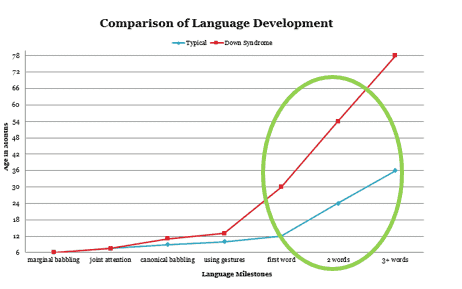
So, it makes sense to not limit our students with Down Syndrome to one communication modality. They truly are unique, and require a variety of interaction options to perform to the best of their abilities. Using this chart, we see that, depending on your goal, different communication outputs or combinations of communication would result in very different outcomes.
If you want to learn more about this topic and also want continuing education, check out our course:

Language Intervention for School-age Children with Down Syndrome
References:
Clibbens, J. (2001). Signing and lexical development in children with Down syndrome. Down Syndrome Research and Practice, 7(3), 101-105.
Early Intervention. National Down Syndrome Society. www.ndss.org
Fidler, D., Most, D. & Philosfsky, A. (2008). The Down syndrome behavioural phenotype: Taking a developmental approach. Down Syndrom Research and Practice. www.down-syndrome.org/research
Foreman, P. & Crews, G. (1998). Using augmentative communication with infants and young children with Down syndrome. Down Syndrome Research and Practice 5(1), 16-25.
Grouios, G. & Ypsilanti, A. (2011). Language and Visuospatial Abilities in Down Syndrome Phenotype: A Cognitive Neuroscience Perspective. www.intechopen.com
Kumin, L. (2012a). Speech and language therapy for children and adolescents with Down syndrome. National Down Syndrome Society. www.ndss.org
Kumin, L. (2012b). Speech and language therapy for infants, toddlers and young children. National Down Syndrome Society. www.ndss.org
Roberts, J., Chapman, R. & Warren, S. (2008). Speech and language development and intervention in Down syndrome and Fragile X Syndrome. Baltiomre, MD: Brookes Publishing
Romski, M. & Sevcik, R. (2005). Augmentative communication and early intervention: Myths and realities. Infants & Young Children, 18(3), 174-185.
Rondal, J. & Buckley, S. (2003). Speech and Language Intervention in Down Syndrome. London: Whurr Publishers Ltd
